.png?width=50&height=50&name=Favicon%20(1).png)
The Centers for Medicare & Medicaid Services (CMS) has released its Calendar Year 2026 Proposed Physician Fee Schedule. While the proposal contains several promising developments for Remote Physiologic Monitoring (RPM) and Chronic Care Management (CCM), it stops short of fully embracing the American Medical Association (AMA) recommendations that many in the industry hoped would modernize and simplify time-based care management billing.
Key Proposed Code Changes: Emphasizing Flexibility and Access
New RPM Code for 2–15 Days of Transmission
A new code, provisionally labeled 99XX4, would allow billing for as few as 2 days of transmission per 30-day period, at the same rate as 99454. This development reflects real-world usage and HealthSnap’s Data Dose model, which emphasizes the clinical value of fewer but meaningful data transmissions.
New 10-19 Minute RPM Management Code
CMS also proposes a 10-19 minute RPM management code (99XX5) with an RVU of 0.31, equivalent to half of the reimbursement of the 20-minute codes. This code would cover clinically relevant interventions that fall short of the 20-minute threshold, such as responding to an alert, reviewing data, or adjusting medication. Though CMS reduced the RVU compared to AMA’s recommendation, its inclusion is a positive development for care teams.
CMS Seeks Data to Sustain 99454
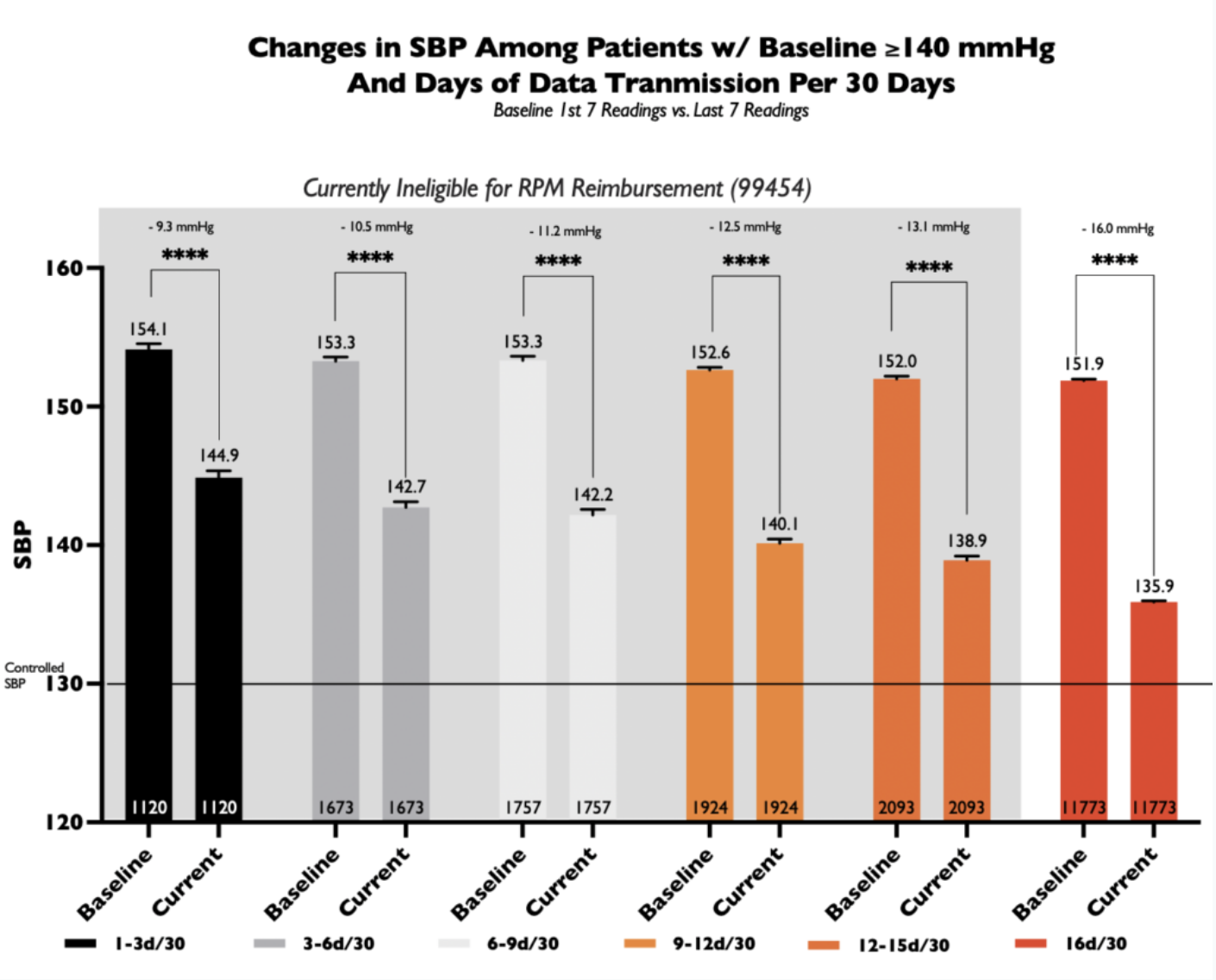
In light of proposed payment reductions for 99454, CMS requests more evidence showing that RPM supply and transmission improve outcomes and reduce costs. Stakeholders are encouraged to submit data linking transmission frequency with cost savings and clinical improvement.
HealthSnap's Data Dose White Paper and the Value of Granular Monitoring
Our white paper, “Fewer Data Points, More Insight,” showed that significant improvements in blood pressure and glucose control can occur with as few as 3–5 days of monthly transmission—as long as data is clinically actionable.
The proposed 2–15 day billing option supports broader use of RPM among:
- Metabolically improving patients
- Post-acute care transitions
- Patients ramping up engagement
- Individuals on GLP-1 therapy where weekly or biweekly weight measurements are clinically sufficient
- Use cases involving physiological parameters—like body weight or pulse oximetry—that require fewer data points to inform care decisions
Longitudinal RPM: A Sustained Framework for Chronic Care
CMS reaffirmed that RPM is not a short-term service:
"CMS considers RPM a longitudinal service, not a short-term episode. It can continue as long as medical necessity exists."
This aligns with HealthSnap’s article on Remote Physiologic Monitoring (RPM) as a Sustained Longitudinal Intervention, which found that patients in RPM for >18 months had 50% higher rates of hypertension control than those in the program <3 months.
Deep Dive: Understanding the Full Scope of Proposed RPM/CCM Changes
To guide stakeholders, we summarize the key CY 2026 proposed code changes and highlight where CMS and AMA are aligned, and where they diverge:
|
Code |
Description |
Current Requirements |
AMA Recommendation |
CMS Proposed Rule |
Outcome/Impact |
|
99454 |
RPM device supply & data transmission |
≥16 days in a 30-day period |
Maintain 99454; Add new code for <16 days |
Move from PE RVU to OPPS data to calculate reimbursement rate |
CMS doesn’t specify a new rate for RPM code 99454, but proposes replacing the PE RVU with OPPS cost data |
|
99XX4 |
(New) RPM 2–15 days code |
No billable option <16 days |
New code at the same rate as 99454 |
Accepted proposal |
Enables broader billing |
|
99457 |
RPM treatment management – first 20 minutes |
≥20 min, incl. interactive time |
Revise to 11–20 minutes |
CMS rejects revision; keeps ≥20 min |
CMS maintains the existing threshold |
|
99458 |
Each additional RPM 20 min |
Each 20 minutes beyond 99457 |
Revise to an additional 10 minutes |
CMS rejects revision; keeps 20 min |
CMS maintains the existing threshold |
|
99XX5 |
(New) RPM management – first 10-19 minutes |
No existing short-duration code |
Suggested with higher RVU |
Accepted but with reduced RVU (0.31) |
CMS values lower than AMA proposed |
|
99490 |
CCM: Non-complex, 20 min of care coordination |
≥20 min/month |
No change |
No change |
Neutral |
|
99487/89 |
Complex CCM: Base (60 min) + add-on (30 min) |
≥60 min + additional time for complex pts |
No change |
No change |
Neutral |
|
99439 |
CCM add-on: each additional 20 min (non-complex) |
+20 min beyond 99490 |
No change |
No change |
Neutral |
|
APCM |
Advanced Primary Care Management |
Holistic longitudinal care payment |
Expand RPM/CCM integration |
Mentioned only |
No integration yet |
AMA vs. CMS: Diverging Paths on Time-Based RPM Codes
Although the AMA has formally approved updates to RPM treatment management codes, such as changing 99457 to cover 11–20 minutes and 99458 to reflect each additional 10 minutes; CMS has rejected these changes in the CY 2026 proposed rule.
Instead, CMS proposes:
- Retaining the current threshold of ≥20 minutes for 99457 and ≥20 minutes for 99458.
- Assigning a lower RVU (0.31) than AMA proposed for the new 10-19 minute code (99XX5).
CMS explains that its decision is due to insufficient survey data and a desire to maintain relativity between RPM and RTM codes. The agency will reassess once utilization data becomes available in 2026.
The Case for Physical Activity as an RPM Vital Sign
CMS’s prevention strategy, including proposed enhancements to the Medicare Diabetes Prevention Program, reflects a growing emphasis on coaching, behavior modification, and evidence-based lifestyle interventions. In alignment with this shift, HealthSnap recommends that CMS formally recognize physical activity as a clinical vital sign, consistent with the CDC’s 2022 analysis of the Physical Activity Vital Sign (PAVS):
“No other basic sign or symptom provides as much information about a patient’s health status as physical activity.”
To operationalize this concept within Medicare payment policy, HealthSnap proposes the following:
- Amend CPT code 99454 to include validated remote monitoring of physical activity metrics (e.g., step count, moderate-to-vigorous physical activity).
- Establish new RPM-like codes for preventive monitoring in patients with cardiometabolic risk.
- Introduce reimbursable codes for patient communication with credentialed lifestyle specialists, including kinesiologists, licensed nutritionists, and certified health coaches.
These recommendations would enable clinicians to proactively manage conditions such as obesity, frailty, arthritis, COPD, and cognitive decline, while reinforcing CMS’s goals of shifting care upstream toward prevention.
As part of its response to the current CMS Request for Information on enhancing prevention, HealthSnap may respond to the RFI with recommendations, such as:
- Creation of a dedicated physical activity RPM code
- Inclusion of metrics derived from FDA-cleared or validated wearable devices
- Alignment with CDC-recommended activity thresholds, such as the 150 minutes/week benchmark
- Inclusion of physical activity, nutrition counseling, and health coaching, delivered through digital or hybrid care models, under new APCM-supported codes
These updates would modernize Medicare's approach to preventive care and support more equitable, scalable access to behavior-based interventions.
Conclusion: A Mixed But Important Step Forward
The CY 2026 CMS proposed rule contains encouraging flexibility in some areas, especially new codes for shorter RPM durations and brief management; but stops short of endorsing the full AMA-backed modernization of time-based RPM billing.
We support:
- Recognition of RPM as longitudinal care
- The new 2–15 day and 10-19 minute RPM codes
- Opportunities to elevate prevention through physical activity monitoring
But we note:
- A significant misalignment with AMA-approved revisions to 99457/99458
- Ongoing reimbursement concerns for 99454
- A continued need for high-quality outcomes data
HealthSnap will continue leading with data, supporting CMS’s goals, and advocating for scalable, equitable reimbursement structures for digital care.
This blog reflects HealthSnap’s initial impressions and will be updated pending the final CMS ruling.




